 Skip to content
Skip to content 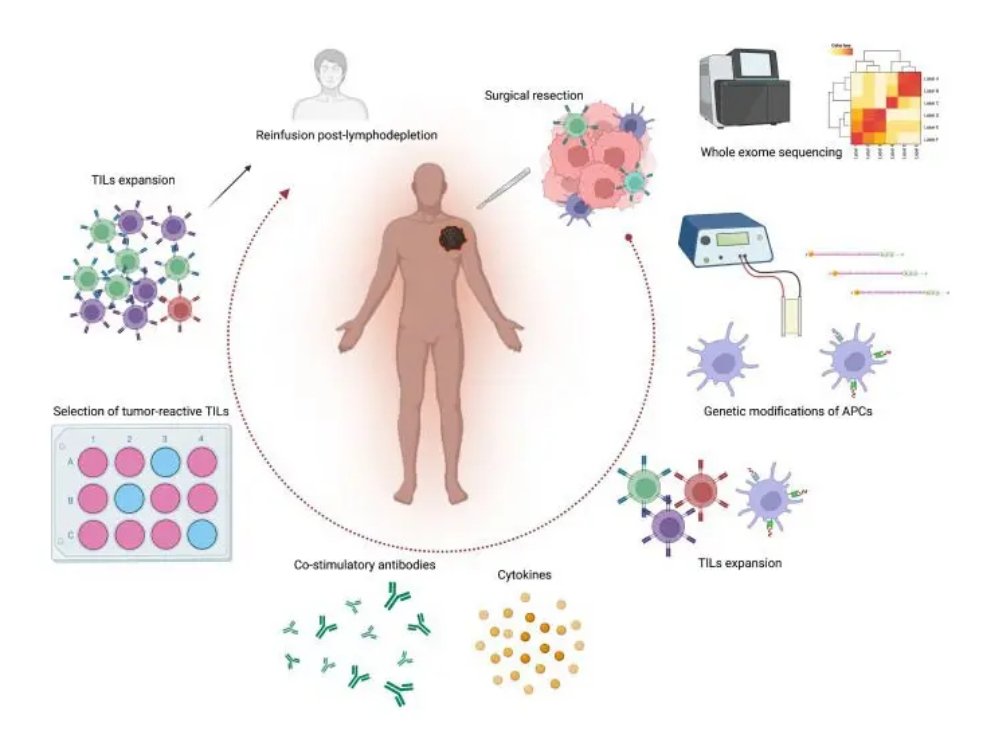
Tumor-Infiltrating Lymphocyte (TIL) therapy is an innovative cancer treatment leveraging a patient’s own immune cells to combat tumors. It has shown promise especially for advanced melanoma and is expanding into other solid tumors. This blog explores the fundamentals, procedure, advantages, indications, TIL extraction sources, patient eligibility, and side effects of TIL therapy.
What is TIL Therapy?
TIL therapy is a personalized form of cellular immunotherapy that uses immune cells called tumor-infiltrating lymphocytes (TILs) harvested directly from a patient’s tumor. These lymphocytes, predominantly T-cells, have naturally migrated into tumors and can recognize and attack cancer cells. After surgical removal of tumor tissue, TILs are isolated and expanded in the lab to billions of highly active cancer-fighting cells. These are then infused back into the patient to target and destroy cancer.
TIL Therapy Procedure
The process begins with surgical removal of a small tumor sample, which is then sent to a lab for TIL extraction. In the lab, TILs are multiplied extensively over several weeks with specialized growth factors. Meanwhile, the patient undergoes a short chemotherapy regimen to suppress their existing immune cells and make room for the incoming TILs. Once the TILs reach sufficient numbers, they are infused back into the patient intravenously. To boost their activity and proliferation, patients receive interleukin-2 (IL-2), an immune-stimulating protein, for several days post-infusion. Recovery typically follows in a few days, with ongoing monitoring.
Advantages of TIL Therapy
- Highly specific and natural: Since TILs are isolated directly from the tumor, they are inherently designed to recognize the patient’s unique cancer markers.
- Polyclonal response: TIL therapy targets multiple tumor antigens simultaneously, reducing the risk of tumor escape through mutation.
- Potential for long-lasting remission: TILs generate memory cells that can continually patrol for and attack cancer cells, offering durable protection.
- Fewer off-target effects: Because TILs are patient-specific and not genetically modified, the risk of damaging healthy tissues is lower than other therapies.
- Single treatment: The therapy is often a one-time infusion, unlike ongoing systemic therapies.
Indications for TIL Therapy
Tumor-infiltrating lymphocyte (TIL) therapy represents a breakthrough in adoptive cell therapy, primarily indicated for patients with advanced or metastatic melanoma who have failed to respond to conventional treatments, including immune checkpoint inhibitors such as anti-PD-1/PD-L1 and anti-CTLA-4 antibodies. The FDA approved lifileucel (Amtagvi) in February 2024 as the first TIL therapy for unresectable or metastatic melanoma after progression on immunotherapy and targeted therapy when applicable.
Beyond melanoma, TIL therapy is under active clinical investigation for multiple solid tumor types. Current trials are evaluating its efficacy in head and neck squamous cell carcinoma, non-small cell lung cancer, cervical cancer, renal cell carcinoma, and other genitourinary malignancies. The therapy shows particular promise in tumors with high mutational burden and robust immune infiltration.
Patient selection criteria are stringent and require tumors accessible for surgical biopsy or resection. Candidates must have adequate performance status (typically ECOG 0-1) and sufficient organ function to withstand the intensive treatment protocol, including lymphodepleting chemotherapy and high-dose interleukin-2 (IL-2) administration. Patients should have measurable disease and life expectancy of at least 3-4 months.
Tissues Used for TIL Extraction
TIL extraction requires fresh tumor tissue obtained through surgical resection or core biopsy procedures. The tissue must be processed within 24-48 hours of collection to maintain lymphocyte viability. Optimal tumor samples are typically 1-3 cm³ in volume, though smaller samples may suffice depending on lymphocyte density.
Primary melanoma lesions, lymph node metastases, and visceral metastases from sites including lung, liver, subcutaneous tissue, and brain have all been successfully used for TIL extraction. In non-melanoma cancers, tissues from primary tumors and metastatic sites in head and neck regions, lung parenchyma, and genitourinary organs have shown successful TIL cultivation.
The extraction process involves either enzymatic digestion using collagenase and DNase or mechanical dissociation to release TILs from the tumor matrix. The harvested cells undergo initial culture in IL-2-containing media to promote T-cell expansion while maintaining tumor reactivity. Quality control measures ensure the final product meets specifications for cell viability, sterility, and functional activity.
Patient Eligibility for TIL Cultivation
Successful TIL cultivation depends on multiple factors beyond initial tissue acquisition. The tumor microenvironment must contain sufficient viable, functionally competent T lymphocytes capable of robust ex vivo expansion. Tumors with high immune infiltration and lower immunosuppressive factors generally yield better TIL cultures.
The cultivation process typically requires 4-6 weeks, during which patients must maintain stable disease to remain eligible for infusion. Progressive disease during this period may exclude patients from receiving treatment. Prior treatments significantly influence cultivation success rates. Patients with recent chemotherapy, radiation therapy, or immunotherapy may have compromised immune function affecting TIL quantity and quality.
Patient immune status, including lymphocyte counts, functional immune markers, and absence of active infections, influences cultivation outcomes. Age, performance status, and concurrent medications also affect the likelihood of successful TIL expansion. Success rates for achieving adequate cell numbers for infusion range from 70-85% in melanoma patients, with variability based on tumor characteristics and patient factors.
Side Effects of TIL Therapy
The toxicity profile of TIL therapy mainly arises from:
- Preparative lymphodepleting chemotherapy (usually cyclophosphamide and fludarabine)
- High-dose IL-2 administration
- Less so from the TIL infusion itself
- High-dose IL-2 administration
Treatment requires hospitalization in specialized centers with intensive care facilities. Immediate post-infusion effects include:
- Constitutional symptoms such as fever, chills, fatigue, and flu-like symptoms within hours of TIL administration
- Respiratory symptoms like dyspnea and cough, especially when combined with IL-2 therapy
- Respiratory symptoms like dyspnea and cough, especially when combined with IL-2 therapy
Hematologic toxicities due to lymphodepletion are universal:
- Severe neutropenia, lymphopenia, and thrombocytopenia typically last 1-2 weeks
- Resulting profound immunosuppression increases infection risk
- Requires prophylactic antimicrobials and close monitoring for bacterial, viral, or fungal infections
- Resulting profound immunosuppression increases infection risk
IL-2-related toxicities include:
- Capillary leak syndrome characterized by increased vascular permeability causing hypotension, fluid retention, and potential end-organ dysfunction
- Cardiovascular effects including arrhythmias, myocardial dysfunction, and hypotension that may need vasopressor support
- Pulmonary toxicity such as pulmonary edema or acute respiratory distress syndrome (ARDS)
- Cardiovascular effects including arrhythmias, myocardial dysfunction, and hypotension that may need vasopressor support
Additional serious adverse events include acute kidney injury, hepatotoxicity, neurologic effects (confusion, somnolence), skin toxicity, and gastrointestinal symptoms. Tumor lysis syndrome may occur in patients with high tumor burden. Conclusion
TIL therapy represents a groundbreaking personalized immunotherapy harnessing the body’s own tumor-fighting cells. With advantages of specificity, durability, and often a single treatment course, it offers hope against difficult-to-treat cancers. Ongoing research and clinical trials continue to expand indications and improve patient outcomes in this evolving landscape of cancer immunotherapy.
Conclusion
TIL therapy is a promising step forward in cancer treatment, offering a personalized way to fight tough cancers by using the body’s own immune cells. While it is still being studied and improved, this approach gives new hope to patients who need better options. With ongoing research and growing success in clinical trials, TIL therapy could soon become an important part of cancer care, marking the start of a new era in treatment.
